The Flipped Food Pyramid
A Clinical Perspective on Why Grains Are No Longer Foundational
My interest in nutrition from a clinical perspective began in 2016, when I first researched the ketogenic way of eating. What started as an exploration of keto for weight loss quickly broadened into something far more substantial. The ketogenic diet was not designed as a lifestyle trend; it originated as a medical intervention for epilepsy, and its effects on metabolism, neurological function, inflammation, and psychological health have been documented for over a century.
That wider therapeutic potential is explored in the documentary The Magic Pill, which illustrates how carbohydrate restriction has been used to support a range of metabolic and neurological conditions. Since then, my ongoing clinical interest has been reinforced by the work of practitioners and researchers such as Dr Sarah Hallberg, Dr Eric Berg, Dr Aseem Malhotra, Professor Tim Noakes, Dr Jason Fung, and Dr Zoe Harcombe, among others. Across different disciplines, the same conclusion repeatedly emerges: significant health improvements are often seen when dietary carbohydrate is reduced and metabolic health is prioritised.
This context matters when we look at the new, flipped U.S. food pyramid.
What the flipped pyramid communicates clinically
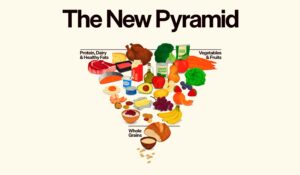
Food pyramids are symbolic tools. They are not neutral. The widest section communicates “most important”; the narrowest communicates “least essential”.
In the flipped pyramid, grains and high-carbohydrate foods sit at the narrow base, while protein, fats, dairy, fruit and vegetables occupy the broader upper levels. From a clinical standpoint, this represents a meaningful shift. It signals that grains are no longer considered foundational to human nutrition.
This aligns far more closely with human physiology than previous grain-heavy models.
Essential nutrients versus optional fuels
In nutritional science, an essential nutrient is one that must be obtained from the diet because the body cannot synthesise it. Humans require:
-
essential amino acids (protein)
-
essential fatty acids (fat)
-
vitamins and minerals
There is no essential carbohydrate. The human body can maintain blood glucose through endogenous mechanisms such as gluconeogenesis and can function efficiently on fat and ketones when carbohydrate intake is low. This is not ideological; it is established metabolic biology.
Carbohydrates may be used as an energy source, but they are not biologically required. (Although some body builders may still feel they need to fuel up – but do your own research for your own body).
Metabolic context matters
In ancestral and pre-industrial contexts, carbohydrate intake was variable, seasonal, and paired with high levels of physical activity. In modern environments, carbohydrate exposure is:
-
constant
-
predominantly refined
-
highly processed
-
metabolically demanding
For individuals with insulin resistance, metabolic syndrome, or type 2 diabetes, a grain-centred diet can perpetuate hyperglycaemia and hyperinsulinaemia. From this perspective, the downgraded position of grains in the flipped pyramid reflects growing recognition of metabolic heterogeneity — not everyone tolerates carbohydrates well, and many are harmed by excessive intake.
Re-centering protein and fat
The elevation of protein and fat within the pyramid restores nutrients that are structurally and hormonally essential. Protein supports muscle mass, immune competence, neurotransmitter production, and tissue repair. Dietary fats contribute to cellular membranes, hormone synthesis, neurological health, and stable energy supply.
From a clinical lens, these are foundational nutrients, not discretionary ones.
The role of plants without carbohydrate dominance
Importantly, the pyramid places fruit and vegetables alongside protein, not as carbohydrate staples but as micronutrient-dense, fibre-rich foods. This distinction matters. A lower-carbohydrate approach does not exclude plants; it prioritises non-starchy vegetables over refined grains and sugars.
A quiet but important correction
The flipped food pyramid does not explicitly advocate a ketogenic or low-carbohydrate diet. However, its visual hierarchy delivers a clear correction to decades of messaging:
-
Grains are not essential
-
Protein and fats are
-
Carbohydrates are contextual and optional
Clinically, this reframing supports a more individualised, metabolically informed approach to nutrition — one that aligns with both physiology and emerging therapeutic evidence.
The question it leaves us with is a simple but necessary one: If grains are not essential, why have they been treated as the foundation of human nutrition for so long?
Disclaimer: this is not a substitute for your own personal research.
Here are scientific links to studies and reviews that support various aspects of ketogenic and low-carbohydrate research — including clinical effects, epilepsy treatment, metabolic health, and the non-essential nature of dietary carbohydrate:
Ketogenic Diet: Clinical Evidence
-
Ketogenic diet overview and mechanisms – comprehensive medical review from StatPearls detailing metabolic effects, clinical applications (epilepsy, type 2 diabetes, obesity), and physiological basis of ketosis. Ketogenic Diet – StatPearls (NCBI)
-
Epilepsy and KD evidence – systematic evaluations showing seizure frequency reductions with ketogenic dietary therapies.
-
Review of KD’s broader neurological roles – evidence on ketogenic diet’s metabolic impacts across neurologic conditions. Impact of the Ketogenic Diet on Neurological Diseases (MDPI)
-
Umbrella review of KD health outcomes – summarises evidence that ketogenic diets are associated with benefits in seizures and cardiometabolic parameters (weight, glucose, lipids) while noting areas needing more long-term trials. Effects of ketogenic diet on health outcomes: umbrella review (BMC Medicine)
Metabolic and Obesity Research
-
RCT evidence on low-carbohydrate vs low-fat diets – large clinical trial showing differences in metabolic outcomes over two years; supports the metabolic impact of carbohydrate restriction. Application of nutrient essentiality criteria to dietary carbohydrates (Cambridge)
-
Ketogenic diet and type 2 diabetes/metabolic syndrome – studies showing improvements in glycaemic control and insulin sensitivity with ketogenic or very-low-carb diets.
Carbohydrate Essentiality
-
Is dietary carbohydrate essential? – exploration of nutrient essentiality criteria showing carbohydrate is not classified as an essential nutrient in humans, unlike fats and amino acids. Is dietary carbohydrate essential for human nutrition? (AJCN)
Supporting Evidence on Mechanism and Effects
-
Ketogenic diet use and contraindications – clinical review outlining physiological effects, including potential metabolic uses beyond epilepsy. Scientific evidence underlying contraindications to the ketogenic diet (NCBI)
-
Clinical evidence for KD in psychiatric and metabolic conditions – emerging human study on effects of ketogenic diets in metabolic and psychiatric outcomes. Ketogenic diet intervention on metabolic and psychiatric measures (ScienceDirect)